


Table of Contents
- Quick Takeaway
- Introduction
- What Is the Nipah Virus and Why Is It a Medical Emergency in India?
- Historical Context of Nipah Virus and Its Public Health Impact
- Nipah Virus 2026 in India: Current Situation, Monitoring, and Health Alerts
- Nipah Virus Symptoms: Early, Advanced & Emergency Signs
- How Is Nipah Virus Diagnosed in India? (With Tests, Labs & Challenges)
- Care, Prevention, and Common Myths About Nipah Virus
- Why Medical Bills Spike During Infectious Disease Outbreaks
- Nipah Virus Treatment and Emergency Medical Support in India
- Conclusion
- FAQs
Quick Takeaway
- Nipah virus has triggered renewed health alerts in India in 2026.
- It is a rare but severe zoonotic disease with a high fatality rate and no specific curative treatment.
- Early symptoms are often non-specific, making timely diagnosis, isolation, and medical monitoring critical.
- Outbreaks place sudden pressure on healthcare systems due to ICU needs, infection-control measures, and prolonged hospital stays.
- Awareness, prevention, and access to timely medical care play a key role in reducing risk to families and communities.
Introduction
Nipah virus 2026 has once again put India on high alert, with suspected and confirmed cases prompting urgent health advisories across multiple states. Known for its unusually high fatality rate, Nipah is not just a medical crisis; it often becomes an unexpected emotional and financial shock for families.
This blog explains what the Nipah virus is, how it spreads, the early warning symptoms people often overlook, and how the disease is diagnosed and managed in India. It also highlights why staying informed through verified health sources is critical during outbreaks, helping individuals and families respond quickly and responsibly.
What Is the Nipah Virus and Why Is It a Medical Emergency in India?
Nipah virus (NiV) is caused by a paramyxovirus first identified in 1998. It has since caused sporadic but deadly outbreaks in South and Southeast Asia, including India.
The virus is primarily carried by fruit bats (Pteropus species), which act as natural reservoirs. Human infection can occur through:
- Direct contact with infected bats or animals
- Consumption of contaminated food (such as fruit or raw date palm sap)
- Human-to-human transmission, especially in healthcare and household settings
What makes the Nipah virus particularly dangerous is its ability to cause acute encephalitis (brain swelling) and severe respiratory illness. Symptoms can worsen rapidly, making early recognition and isolation critical to prevent complications and further spread.
Why Nipah Virus Has a High Fatality Rate
While data suggests outcomes vary by outbreak and healthcare access, the Nipah virus has historically shown a case fatality rate ranging from 40% to 75%, significantly higher than most common viral infections.
Factors contributing to severity include:
- Rapid neurological involvement
- Absence of a specific antiviral treatment
- Delayed symptom recognition
- High risk of complications in critical cases
Quick Answer: Nipah virus is a rare but severe zoonotic infection that spreads from animals to humans and can also be transmitted between people. In India, the Nipah virus causes acute fever, brain inflammation, and respiratory distress, often requiring immediate hospital isolation and intensive care due to its high fatality rate.
Historical Context of Nipah Virus and Its Public Health Impact
Nipah virus was first identified in Malaysia in 1998, when an outbreak among pig farmers led to widespread illness and significant loss of life. Subsequent investigations confirmed fruit bats (Pteropus species) as the natural reservoir, establishing Nipah as a high-risk zoonotic infection capable of transmitting from animals to humans. This discovery marked Nipah as a serious global health concern due to its ability to cause severe neurological disease and rapid clinical deterioration.
India reported its first Nipah virus outbreak in 2001 in West Bengal, followed by additional clusters in later years. A major turning point occurred in 2018, when a severe outbreak in Kerala demonstrated how quickly the virus could spread within households and healthcare settings, even when initial case numbers were small. Since then, sporadic cases and surveillance alerts have continued to emerge, particularly in southern and eastern regions of the country. Each new cluster has triggered swift containment and monitoring efforts, reinforcing Nipah’s status as a recurring yet unpredictable public health threat, rather than a one-time outbreak.
Scale and Severity: What 25 Years of Nipah Virus Outbreaks Reveal
Over the past 25 years, Nipah virus outbreaks have been documented across multiple countries. Although the total number of cases has often remained limited, the outcomes have been consistently severe:
- Total impact (as of May 2024): 754 confirmed human Nipah virus cases with 435 deaths across five countries ( Case Fatality Rate – CFR: 58%)
- Bangladesh: 341 cases and 241 deaths, the highest recorded burden (CFR: 71%)
- Malaysia: 283 cases and 109 deaths during the initial major outbreak (CFR: 39%)
- India: 102 cases and 74 deaths reported across multiple outbreak clusters (CFR: 73%)
- Philippines & Singapore: Smaller outbreaks under strict surveillance — Philippines (17 cases, 9 deaths; CFR: 53%) and Singapore (11 cases, 1 death; CFR: 9%)
These figures highlight a defining feature of the Nipah virus: even relatively small outbreaks can result in a disproportionately high number of deaths, particularly when diagnosis, isolation, or supportive care is delayed.
Quick Answer: Nipah virus was first identified in 1998 and has since caused recurring outbreaks across South and Southeast Asia. Globally, Nipah is recognised as a high-fatality zoonotic disease with limited treatment options, prompting strict surveillance, rapid isolation protocols, and ongoing research into prevention and outbreak control.

Nipah Virus 2026 in India: Current Situation, Monitoring, and Health Alerts
Current Nipah Virus Situation in India (2026)
As of 2026, the Nipah virus remains a priority public health risk for Indian health authorities, who continue to treat it as such, especially during periods when suspected or confirmed cases are reported. While outbreaks remain limited in scale, even isolated cases trigger heightened monitoring and containment measures due to Nipah’s rapid progression and potential for human-to-human transmission.
States that have reported Nipah virus cases in the past, such as Kerala and West Bengal, remain under closer epidemiological watch. Other regions, including parts of southern and eastern India, are also included in routine surveillance based on ecological and historical risk patterns.
Rather than widespread transmission, the current concern lies in early detection, containment, and prevention of secondary spread, particularly within households and healthcare settings.
Government and Health Authority Response
During suspected or confirmed Nipah virus alerts, Indian health authorities typically implement:
- Rapid response teams for case investigation
- Isolation wards in designated government hospitals
- Contact tracing and monitoring of high-risk exposures
- Temporary containment zones, if required
- Public health advisories for hospitals and communities
The Indian Council of Medical Research (ICMR) and state health departments coordinate testing, clinical guidance, and reporting to ensure consistency and accuracy during evolving situations.
Healthcare Preparedness and Testing Capacity
India’s preparedness for Nipah virus isolation and hospital care has improved following past outbreaks. Many tertiary care government hospitals now maintain protocols for:
- Suspected case triaging
- Sample collection and transport to approved laboratories
- Strict infection-control practices for healthcare workers
- Monitoring patients with neurological or respiratory symptoms
However, challenges may still arise during alerts, including limited testing centres, high demand for isolation beds, and the need for specialised critical care support.
Quick Answer: In 2026, the Nipah virus in India remains under close surveillance due to its history of high fatality rates and sudden outbreaks. Health authorities monitor suspected cases through rapid testing, isolation protocols, and contact tracing, particularly in states with previous outbreaks, to prevent community transmission.
Nipah Virus Symptoms: Early, Advanced & Emergency Signs
Early Nipah Virus Infection
Nipah virus infection often starts with general symptoms that can mimic common viral illnesses, making early detection challenging. The typical incubation period (time from exposure to first symptoms) is about 4–14 days, though longer intervals have been reported.
Early warning signs include:
- Fever and chills
- Headache and muscle aches
- Sore throat or coughing
- Fatigue or unusual weakness
- Nausea, vomiting, or gastrointestinal discomfort
These early symptoms can resemble common flu or viral infections, which is why high suspicion and quick medical assessment are important, especially if exposure risk exists.
Advanced Nipah Virus Symptoms: Progression to Serious Illness
As the infection progresses, particularly without prompt medical attention, respiratory and neurological involvement can occur:
Progressive or severe signs include:
- Breathing difficulties or rapid respiratory decline
- Pneumonia or severe respiratory distress
- Dizziness, drowsiness, or altered consciousness
- Confusion or disorientation
- Seizures indicating acute encephalitis (brain inflammation)
In the most severe cases, encephalitis can develop, causing neurological complications that may lead to coma within 24–48 hours.
Emergency Signs: When to Seek Immediate Care
Seek urgent medical help or go to a hospital immediately if any of the following occur:
- Sudden confusion or inability to remain awake
- Seizures or unresponsiveness
- Severe shortness of breath
- Weakness progressing rapidly
- Coma or collapse
These are medical red flags suggesting severe involvement of the brain or lungs and require immediate hospital care, especially in outbreaks or exposure scenarios.
Quick Answer: Nipah virus symptoms typically begin with non-specific flu-like signs such as fever, headache, and fatigue, and can progress within days to severe respiratory distress or encephalitis, including confusion, seizures, and coma. Early recognition and medical evaluation are critical for possible isolation and supportive care.
How Is Nipah Virus Diagnosed in India? (With Tests, Labs & Challenges)
Nipah virus infection is diagnosed through a combination of clinical assessment and specialised laboratory tests. Because early symptoms often resemble common viral illnesses, laboratory confirmation is key to triggering isolation, outbreak response, and contact tracing.
Diagnostic Tests Used for Nipah Virus
1. RT-PCR (Reverse Transcription Polymerase Chain Reaction)
This is the primary and most reliable test for detecting active Nipah virus infection. It identifies viral RNA in clinical samples and is the cornerstone of acute diagnosis. Samples may include:
- Throat and nasal swabs
- Blood
- Cerebrospinal fluid (CSF)
- Urine
RT-PCR allows detection during the early phase of illness and supports rapid confirmation.
2. ELISA (Antibody Detection Tests)
Enzyme-linked immunosorbent assay (ELISA) detects IgM and IgG antibodies against Nipah virus:
- IgM ELISA suggests recent infection
- IgG ELISA indicates past exposure or later stages of infection
Antibody tests are useful when symptoms have progressed or when the viral load declines below detection by PCR.
3. Virus Isolation & Serological Panels
In specialised settings, virus isolation, serum neutralisation tests, and advanced serology can be used for outbreak investigation and confirmation at reference laboratories, although these are not routine for immediate clinical decision-making.
Where Testing Is Available (GEO-Focused for India)
In India, Nipah virus testing is available at designated public health laboratories that meet biosafety standards for high-risk pathogens:
- National Institute of Virology (NIV), Pune — National reference centre for confirmatory RT-PCR and serology.
- State Virus Research & Diagnostic Laboratories (VRDLs) — Provide preliminary testing and sample handling.
- Recent expansions include mobile testing labs and local capacity upgrades in cities such as Kolkata, improving turnaround times and outbreak response.
Private hospitals often send samples to these designated testing centres when on-site facilities are unavailable, and results may take several days depending on logistics and capacity.
Why Early Detection Reduces Risk to Families and Communities
Early diagnosis matters for three key reasons:
- It enables immediate isolation of confirmed cases to reduce onward transmission.
- It helps health teams initiate contact tracing and monitoring of exposed individuals.
- It supports quicker medical evaluation and supportive care, which can influence outcomes and reduce spread within households and healthcare settings.
Delays in testing, due to limited local capacity or logistical hurdles, can prolong uncertainty and increase the risk of community spread. Strengthening local lab readiness and sample transport systems remains a priority during outbreak response.
Challenges: Limited Testing Capacity During Outbreaks
Although India has expanded diagnostic capacity, several limitations persist:
- Fewer high-containment labs with BSL-3/BSL-4 capabilities are required for safe handling of Nipah samples.
- Dependence on centralised facilities for confirmatory RT-PCR can delay reporting.
- Transport and cold-chain requirements for samples from remote regions to reference labs, especially during alerts.
Efforts to decentralise testing and deploy rapid diagnostic technologies are ongoing, but challenges remain, particularly during sudden increases in suspected cases.
Quick Answer: In India, Nipah virus diagnosis relies on RT-PCR to detect viral RNA and ELISA antibody testing to confirm infection stages. Samples are processed at designated high-containment labs such as NIV Pune and state VRDLs. Early detection enables isolation and outbreak control, though limited specialised testing capacity can delay confirmation.
Care, Prevention, and Common Myths About Nipah Virus
Preventing Nipah virus infection relies heavily on awareness and everyday precautions, especially during active surveillance or outbreaks in India. Families are advised to avoid contact with sick or dead animals, particularly bats and pigs, and not consume half-eaten or fallen fruits, which may be contaminated by bat saliva. Practising proper food hygiene, including washing and peeling fruits, remains essential.
In outbreak-prone areas, wearing masks in crowded or healthcare settings, limiting unnecessary travel, and following state health department alerts can reduce exposure risk. Caregivers looking after a suspected or confirmed patient at home should follow strict isolation guidance, avoid direct contact with bodily fluids, and seek medical advice immediately if symptoms appear.
Alongside prevention, addressing misinformation is equally important:
- Myth: Nipah spreads as easily as COVID-19
Fact: Nipah does not spread as rapidly, but human-to-human transmission can occur through close contact, making early isolation critical. - Myth: Only rural areas are at risk
Fact: While initial exposure may occur near animal reservoirs, cases can spread to urban healthcare settings through caregivers and hospital contact. - Myth: Nipah virus symptoms appear immediately.
Fact: Symptoms may take days to appear, which is why monitoring and reporting early signs matter. - Myth: Nipah can be treated at home
Fact: Suspected cases require hospital evaluation and isolation, not home-based treatment.
Clear information, early reporting, and adherence to public health guidance remain the most effective tools for Nipah virus precautions from outbreaks in 2026.
Note: Unlike highly contagious viruses such as COVID-19, the Nipah virus is not easily transmissible. Most human-to-human transmission occurs through close, prolonged contact, particularly in household or healthcare settings.
Why Medical Bills Spike During Infectious Disease Outbreaks
During outbreaks like Nipah, medical costs rise sharply, not because treatment is advanced, but because care becomes resource-intensive and time-sensitive. Hospitals face sudden pressure on critical infrastructure, and families often bear the financial impact.
One major factor is the increased demand for ICU beds. Even suspected cases may require close neurological or respiratory monitoring, which limits bed availability and pushes care toward higher-cost settings. At the same time, hospitals must follow strict infection-control protocols, leading to higher spending on PPE, isolation rooms, sanitisation, and trained staff.
Outbreaks also involve emergency transport, referrals between facilities, and prolonged hospital stays. Patients are often kept under observation longer than usual to prevent complications and community spread, adding to room, testing, and specialist consultation costs.
Nipah Virus Treatment and Emergency Medical Support in India
There is currently no specific antiviral treatment that cures Nipah virus infection; only precautions can be taken. Medical care focuses on early isolation, close monitoring, and intensive supportive treatment to manage complications and reduce the risk of death and further transmission. Patients with neurological or respiratory involvement often require hospitalisation in isolation wards or intensive care units.
Because care relies on critical support rather than curative medication, medical expenses can rise quickly, especially when ICU monitoring, ventilator support, specialised testing, and strict infection-control measures are needed. The urgency of care leaves little time for families to arrange insurance approvals or long-term financial planning.
In such emergencies, some families in India turn to verified medical crowdfunding platforms like ImpactGuru to manage immediate hospital-related expenses. Crowdfunding does not replace medical treatment or guarantee outcomes, but it can help families access timely care without delays during sudden, high-cost infectious disease situations.
Note: This information is based on publicly available data from health authorities and outbreak surveillance reports and does not replace medical advice.

Conclusion
Nipah virus remains one of the most serious zoonotic health threats in 2026 due to its high fatality rate, unpredictable outbreaks, and absence of a specific cure. While cases are relatively rare, past outbreaks across Asia have shown that delayed detection, limited testing access, and strained healthcare infrastructure can quickly escalate risks for patients, families, and frontline workers.
Encouragingly, surveillance, containment protocols, and clinical preparedness have improved over time. However, early medical attention, strict isolation, and critical care support remain essential to limiting transmission and improving outcomes. These measures, while life-saving, often come with significant emotional and financial strain for affected families.
FAQs
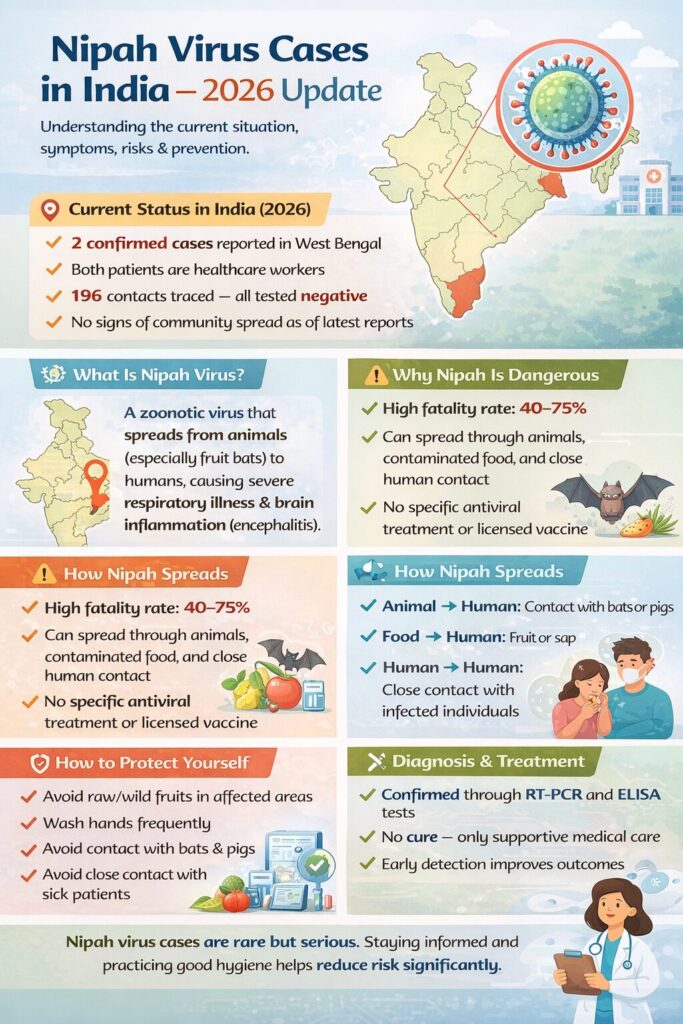
Nipah virus is a zoonotic infection that causes severe respiratory illness and brain inflammation. It spreads from fruit bats, contaminated food, or close human contact.
In 2026, Nipah cases were reported in West Bengal, with two confirmed infections and all close contacts testing negative.
Early symptoms include fever, headache, cough, and breathing difficulty. Severe cases can lead to confusion, seizures, or coma.
Avoid raw fruits, wash hands frequently, avoid contact with bats or pigs, and follow local health advisories and hygiene practices.
There is no specific cure or antiviral treatment. Diagnosis is done through RT-PCR or ELISA tests, and patients receive supportive medical care.










